Imagine reaching up to grab something from a shelf — and your arm simply won’t cooperate. Or trying to button your shirt in the morning and wincing with every small movement. Perhaps you wake at 2 a.m., unable to find a comfortable position because the aching in your shoulder won’t let you rest. If any of this sounds familiar, you are far from alone.
Shoulder pain causes and treatment is one of the most searched health topics for good reason: shoulder pain affects approximately 1 in 3 people at some point in their lives, making it one of the most common musculoskeletal complaints after back and neck pain. It can strike anyone — office workers hunched over keyboards, athletes pushing their limits, homemakers lifting heavy loads, and older adults dealing with years of wear.
In this guide, written by a qualified physiotherapist, you will learn: the most common types of shoulder pain and what causes them; which conditions you can safely manage at home and which need professional physiotherapy; evidence-based home remedies that actually work; vitamins and supplements that support recovery; a step-by-step physiotherapy exercise programme you can do at home; and the warning signs that mean you should seek medical attention without delay.
What Is Shoulder Pain? Understanding the Types of Shoulder Pain
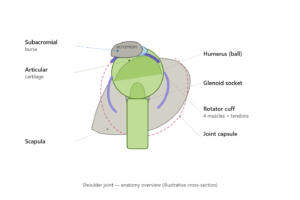
The shoulder is the most mobile joint in the human body. It is a ball-and-socket joint where the head of the upper arm bone (humerus) fits into a shallow socket in the shoulder blade (scapula). Surrounding this joint is the rotator cuff — a group of four muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) — along with a fluid-filled sac called the bursa, the joint capsule, and multiple tendons. This extraordinary range of movement is precisely why the shoulder is so vulnerable to injury and pain.
According to NHS guidance, the most frequent causes of shoulder pain include problems with the rotator cuff, frozen shoulder, and referred pain from the neck or other structures [1].
The 6 Most Common Types of Shoulder Pain
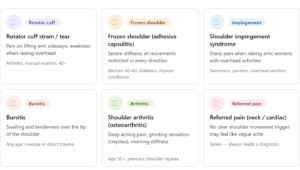
- Rotator Cuff Strain or Tear— The rotator cuff muscles can be strained (overstretched) or torn, either partially or fully. The hallmark symptom is pain when lifting the arm, particularly to the side, often with weakness. It is most common in athletes, manual workers, and people over 40.
- Frozen Shoulder (Adhesive Capsulitis)— The joint capsule thickens and tightens, severely restricting movement in all directions. It progresses through three stages: freezing (intense pain), frozen (stiffness dominates), and thawing (gradual recovery). It disproportionately affects women aged 40–60 and people with diabetes or thyroid conditions.
- Shoulder Impingement Syndrome— The tendons of the rotator cuff become pinched against the acromion (the bony roof of the shoulder) during overhead movements, causing pain and inflammation. Swimmers, painters, and overhead workers are particularly susceptible.
- Bursitis— Inflammation of the bursa sac leads to localised swelling and tenderness, often over the tip of the shoulder. It can be triggered by overuse, a direct blow, or as a secondary feature of impingement.
- Shoulder Arthritis (Osteoarthritis)— Progressive wear of the joint cartilage produces a deep, aching pain, stiffness, and sometimes a grinding sensation (crepitus) with movement. More common in people over 50 and those with previous shoulder injuries.
- Referred Pain from the Neck or Heart— Not all shoulder pain originates in the shoulder. Cervical spine (neck) problems can refer pain into the shoulder and arm. Crucially, cardiac events can also present as left shoulder pain, especially when accompanied by chest tightness, breathlessness, or sweating. If in doubt, seek emergency care immediately.
Shoulder Pain Causes and Treatment: Home Care vs. Physiotherapy
Understanding shoulder pain causes and treatment starts with one critical question: Does your shoulder need rest and home care, or does it need professional physiotherapy? Getting this wrong — particularly resting a condition that needs active treatment — can significantly delay your recovery.
Conditions You Can Manage at Home
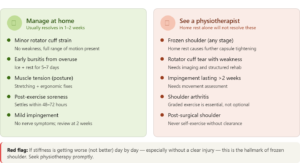
The following conditions respond well to home care when managed promptly and correctly:
- Minor rotator cuff strain (no weakness, full range of motion) — gentle activity modification, ice for the first 48 hours, and relative rest for 5–7 days typically leads to noticeable improvement.
- Early-stage bursitis from overuse — ice, anti-inflammatory pain relief, and temporarily avoiding the aggravating activity (e.g. overhead lifting) for 1–2 weeks usually resolves symptoms.
- Muscle tension from poor posture — stretching, posture correction, and ergonomic adjustments can resolve this within days to weeks.
- Post-exercise soreness (DOMS) — this is normal muscle adaptation and settles within 24–72 hours with rest, hydration, and gentle movement.
- Mild shoulder impingement without nerve symptoms — activity modification, posture awareness, and gentle shoulder exercises can help, but if no improvement occurs within 2 weeks, see a physiotherapist.
Conditions That Require Physiotherapy
The following conditions will not resolve adequately with home rest alone — and attempting to manage them without professional guidance can cause lasting harm:
- Frozen shoulder (any stage) — this is not a condition to rest through at home for months. Physiotherapy is essential to prevent the capsule from tightening further during the freezing stage and to restore range of motion during the thawing stage. Home management alone extends suffering unnecessarily and increases the risk of permanent stiffness.
- Rotator cuff tear with weakness — if you cannot raise your arm fully or feel genuine weakness, a partial or full tear may be present. This requires imaging and a structured rehabilitation programme.
- Shoulder impingement lasting more than 2 weeks — persistent impingement needs a proper movement assessment and a graded exercise programme to correct the underlying mechanics.
- Post-surgical shoulder — rehabilitation after any shoulder procedure must be guided by a physiotherapist. Independent exercise is inappropriate without clearance.
- Shoulder arthritis — graded, evidence-based exercise is the single most effective non-surgical treatment for shoulder arthritis. It is not optional.
- Recurrent shoulder dislocations — each dislocation increases joint instability. A physiotherapist can prescribe stabilisation exercises that significantly reduce recurrence risk.
“In my clinical experience, the most common mistake patients make is waiting too long. “They rest a frozen shoulder at home for six months, and by the time I see them, the capsule is severely contracted. Early physiotherapy makes a measurable difference to recovery time across almost every shoulder condition.”
Shoulder Pain Home Remedies That Actually Work
For the conditions listed above that are appropriate for home management, the following evidence-informed remedies can provide meaningful relief:
RICE Protocol (First 48–72 Hours for Acute Injuries Only)
Rest the shoulder from aggravating activities. Ice the area for 15–20 minutes every 2–3 hours using a cloth-covered ice pack. Compression is less commonly used at the shoulder but can help with significant swelling. Elevate where possible. Do not apply ice for longer than the recommended time — it can cause ice burns.
Heat Therapy
Warmth is appropriate for chronic stiffness — the frozen shoulder thawing stage, arthritis, and long-standing muscle tension. Apply a warm compress or heat pad for 15–20 minutes before stretching or exercise. Important: Never apply heat to an acute injury or fresh swelling — it increases inflammation.
Ice Therapy
Ice is for acute pain and swelling in the first 2–3 days after injury. Once the acute phase passes, it loses effectiveness. Do not use ice for stiffness — it will make movement more difficult.
Over-the-Counter Pain Relief
Ibuprofen (anti-inflammatory) or paracetamol (analgesic) can help manage pain short-term. Use for a maximum of 5–7 days without medical supervision. Note: ibuprofen is not suitable for people with stomach ulcers, kidney disease, or those on blood-thinning medication. Always read the label.
Sleep Position
Sleeping on the affected shoulder compresses the joint and worsens most shoulder conditions. Try sleeping on your back with a small pillow tucked under the affected arm for support, or on the opposite side. This simple change can significantly reduce night pain.
Posture Correction
Forward head posture and rounded shoulders narrow the subacromial space and directly contribute to impingement. Raise your monitor to eye level, ensure your keyboard allows relaxed shoulders, and take short standing breaks every 30–40 minutes. Even small improvements in posture reduce shoulder loading throughout the day.
Gentle Pendulum Exercises
This is the one exercise safe even during the most painful stage of frozen shoulder. Lean forward, support yourself with your unaffected arm on a table, and let the affected arm hang freely. Gently swing it in small circles — clockwise and anticlockwise — for 30–60 seconds. The movement uses gravity rather than muscle force to gently open the joint capsule.
Vitamins and Supplements for Shoulder and Joint Pain
Supplements can support the body’s healing process — but they are not a cure for structural problems. Treat them as a complement to physiotherapy, not a replacement for it. The evidence for each varies:
Vitamin D3 (Strong evidence) — Vitamin D deficiency is strongly linked to musculoskeletal pain, impaired muscle function, and slower tendon healing. Have your levels tested before supplementing, as dosage depends on your baseline. Deficiency is extremely common, particularly in urban populations with limited sun exposure. [2]
Liposomal Magnesium (Moderate evidence) — Magnesium plays a key role in muscle relaxation and sleep quality. Liposomal forms offer superior absorption. Particularly helpful for patients with significant night pain and muscle tension.
Collagen Type II (Emerging evidence) — Undenatured Type II collagen has shown promise for joint cartilage support, particularly in osteoarthritis. More research is needed, but early findings are encouraging. It is not a cure — think of it as joint maintenance.
Micellar Curcumin + AKBA Boswellia (Mild-moderate evidence) — Curcumin (from turmeric) and Boswellic acid (AKBA form from Boswellia) both have anti-inflammatory properties. Standard curcumin has poor absorption; micellar curcumin addresses this significantly. The AKBA form of Boswellia is the most biologically active. Combined, they may reduce inflammation and pain with continued use. [3]
Liposomal Vitamin C (Moderate evidence) — Vitamin C is essential for collagen synthesis, which means it is directly relevant to tendon and ligament repair. Liposomal delivery improves bioavailability. Particularly worth considering post-injury and post-surgery.
⚕️ Consult your doctor before starting any supplement, especially if you are on blood thinners, have kidney disease, or are pregnant.
When to See a Doctor or Physiotherapist for Shoulder Pain
Think of this section not as a list of alarming symptoms, but as a guide to signs that professional care will meaningfully speed your recovery:
See a Physiotherapist if You Notice:
- Pain that lasts more than 2 weeks with no improvement despite home care
- Inability to raise your arm above shoulder height
- Stiffness that is getting worse, not better (key red flag for frozen shoulder)
- Pain that regularly disturbs your sleep
- A fall, sports impact, or other sudden injury to the shoulder
- A diagnosis of diabetes or a thyroid condition — both significantly increase frozen shoulder risk and require earlier intervention
Seek Emergency Care (A&E) or Urgent Medical Attention if You Have:
- Visible deformity or a suspected dislocation following trauma
- Numbness, tingling, or weakness running down the arm (possible nerve compression)
- Shoulder pain accompanied by chest pain, shortness of breath, or sweating — this can indicate a cardiac event and requires immediate emergency assessment
- Sudden, severe shoulder pain with no obvious cause
Shoulder Physiotherapy Exercises for Pain Relief
The following exercises cover the most common shoulder conditions. Always work within a pain-free or mildly uncomfortable (not sharply painful) range. If an exercise causes sharp or worsening pain, stop immediately.
1. Pendulum Swings
Suitable for: Frozen shoulder (all stages), acute rotator cuff strain
- Stand and lean forward, supporting your unaffected arm on a table or chair.
- Let the affected arm hang down freely.
- Gently swing the arm in small clockwise circles for 30 seconds, then anticlockwise.
- Gradually increase the circle size over days as tolerated.
Sets/Reps: 2–3 minutes, twice daily
Why it helps: Uses gravity and momentum to decompress the joint capsule without muscular effort.
Avoid: Forcing larger movements — let the arm swing naturally.
2. Wall Walk (Finger Walking)
Suitable for: Frozen shoulder Stage 2, shoulder impingement
- Stand facing a wall, arm’s length away.
- Place the fingertips of the affected arm on the wall at waist height.
- Walk the fingers slowly upward as far as comfortable.
- Hold at the top for 3–5 seconds, then walk back down.
Sets/Reps: 3 sets of 10 repetitions, once daily
Why it helps: Gradually improves passive range of motion in a controlled, safe way.
Avoid: Hiking the shoulder upward — keep it relaxed as the fingers walk.
3. Cross-Body Stretch (Posterior Capsule Stretch)
Suitable for: Frozen shoulder Stages 2–3, shoulder impingement
- Bring the affected arm across your chest at shoulder height.
- Use the opposite hand to gently pull the elbow toward your body.
- Hold for 20–30 seconds, breathing steadily.
Sets/Reps: 3 repetitions, 2–3 times daily
Why it helps: Stretches the posterior joint capsule, addressing a key cause of shoulder tightness and impingement.
Avoid: Pulling aggressively — a gentle stretch is sufficient.
4. Sleeper Stretch (Internal Rotation)
Suitable for: Frozen shoulder Stage 3, shoulder impingement, rotator cuff rehabilitation
- Lie on your side on the affected shoulder, with the shoulder at 90 degrees.
- Bend the elbow to 90 degrees so the forearm points upward.
- Use the opposite hand to gently push the forearm downward toward the bed.
- Hold for 20–30 seconds.
Sets/Reps: 3 repetitions, twice daily
Why it helps: Stretches the posterior capsule and improves internal rotation, which is commonly lost in impingement and late-stage frozen shoulder.
Avoid: If this causes sharp pain, stop and consult your physiotherapist first.
5. Towel Stretch (External Rotation Behind Back)
Suitable for: Frozen shoulder Stages 2–3 (thawing phase)
- Hold a rolled towel or belt behind your back — unaffected hand at the top, affected hand at the bottom.
- Use the top hand to gently pull the towel upward, drawing the lower (affected) arm up behind the back.
- Hold at the point of comfortable tension for 20–30 seconds.
Sets/Reps: 3 repetitions, twice daily
Why it helps: Improves external rotation behind the back, which is typically the last movement to return in frozen shoulder recovery.
Avoid: Do not force — progress gently over days.
6. Resistance Band External Rotation
Suitable for: Rotator cuff strengthening, frozen shoulder Stage 3, arthritis rehabilitation
- Anchor a resistance band at elbow height to a door handle or fixed point.
- Stand side-on, affected arm closest to the anchor.
- Hold the band with the elbow bent at 90 degrees and tucked into the side.
- Rotate the forearm outward against the band’s resistance, keeping the elbow in.
- Slowly return to start.
Sets/Reps: 3 sets of 12–15 repetitions, twice daily
Why it helps: Directly strengthens the infraspinatus and teres minor — key rotator cuff stabilisers.
Avoid: Allowing the elbow to flare away from the body during the movement.
7. Scapular Retraction
Suitable for: All shoulder conditions — postural correction
- Sit or stand with arms relaxed at your sides.
- Gently squeeze the shoulder blades together as if pinching a pencil between them.
- Hold for 5 seconds, then release fully.
Sets/Reps: 3 sets of 15 repetitions, twice daily
Why it helps: Activates the lower trapezius and rhomboids, correcting rounded shoulder posture and reducing impingement load.
Avoid: Shrugging the shoulders upward — keep them down and back.
8. Isometric Shoulder Press Against Wall
Suitable for: Early shoulder arthritis, post-injury strengthening (when full movement is not yet available)
- Stand facing a wall with the affected arm bent at 90 degrees.
- Place the back of the hand or forearm against the wall.
- Press gently into the wall without any movement — an isometric contraction.
- Hold for 5–10 seconds, then release.
Sets/Reps: 3 sets of 10 repetitions, twice daily
Why it helps: Builds shoulder strength in a pain-friendly way when active range of motion is limited.
Avoid: Pressing so hard that pain is provoked.
Medical Interventions: An Informational Overview
Some shoulder conditions require medical procedures beyond physiotherapy. The following is an educational overview only — none of these should be self-administered or pursued without a doctor’s evaluation:
Corticosteroid Injections — Used for bursitis, early frozen shoulder, and rotator cuff tendinopathy, these injections reduce inflammation and offer short-term pain relief. They are not a long-term solution — repeated injections can weaken surrounding tendon tissue. Most effective when followed by physiotherapy.
PRP Injections (Platelet-Rich Plasma) — A small amount of the patient’s own blood is processed to concentrate healing growth factors and injected into the affected area. Evidence is growing for rotator cuff tendinopathy and partial tears. PRP is generally well-tolerated as it uses the patient’s own blood, but results vary and it is not universally available on standard health plans.
Hydrodilatation — A mixture of saline, corticosteroid, and local anaesthetic is injected under imaging guidance to stretch the contracted shoulder capsule. Used primarily for frozen shoulder that is not responding adequately to physiotherapy alone. Most effective when combined with immediate physiotherapy follow-up.
Manipulation Under Anaesthesia (MUA) — The shoulder is moved through its full range of motion under general anaesthesia to break down scar tissue. Considered when physiotherapy, injections, and hydrodilatation have not produced sufficient improvement.
Shoulder Replacement Surgery — Reserved for severe osteoarthritis where all other approaches have failed. Recovery requires several months of structured physiotherapy rehabilitation.
All medical procedures listed above require a doctor’s evaluation and prescription. Do not attempt self-treatment for these.
Realistic Recovery Timeline: How Long Does Shoulder Pain Last?
One of the most common questions patients ask is how long recovery will take. The honest answer is: it depends on the condition and whether appropriate treatment is started early.
Minor muscle strain: 1–2 weeks with home care. Physiotherapy rarely needed.
Bursitis: 2–4 weeks with rest and anti-inflammatories. Faster with physiotherapy if impingement is confirmed.
Rotator cuff tendinopathy: 4–12 weeks. Typically 6–8 weeks with guided physiotherapy.
Shoulder impingement: Limited recovery with home rest alone. 6–12 weeks with guided rehabilitation.
Frozen shoulder: 1–3 years if left to self-resolve without treatment. 12–18 months with consistent physiotherapy — and significantly less suffering throughout.
Shoulder arthritis: Ongoing management rather than a defined end point, but outcomes are significantly better with structured exercise and physiotherapy input.
The evidence is consistent: early physiotherapy leads to faster recovery and better long-term outcomes across virtually every shoulder condition. There is rarely a good reason to delay.

