The landscape of orthopaedic and musculoskeletal surgery in India has undergone a seismic shift over the last decade. With advancements in surgical techniques, such as minimally invasive arthroscopy and robotic-assisted joint replacements, the technical success of a procedure is higher than ever. However, a successful surgery is only the midpoint of a patient’s journey. The final outcome—true functional independence—is determined by the quality of post-surgical rehabilitation.
In the Indian clinical context, we frequently encounter a dichotomy in patient attitudes. On one end, there is the misconception that “pain means the exercise is working,” leading to aggressive, unsupervised over-exertion. On the other, cultural factors often lead patients to prioritize a premature return to work or household responsibilities, often at the cost of ignoring necessary physiological healing timelines. Furthermore, the rise of “YouTube-based rehabilitation” has introduced a significant risk, where patients attempt complex maneuvers without understanding the biomechanical stresses placed on healing tissues or implants.
Poorly managed rehabilitation in the early post-operative weeks often results in preventable complications: persistent joint stiffness (arthrofibrosis), muscle atrophy, chronic pain syndromes, and in severe cases, implant failure or the necessity for revision surgery. At Rayara Kirana Physiotherapy, we advocate for a structured, evidence-based approach that respects biological healing while driving functional recovery.
INCIDENCE OF POST-SURGICAL REHABILITATION NEEDS IN INDIA
The demand for post-surgical rehabilitation in India is rising exponentially, driven by an ageing population and an increase in sports-related injuries among the youth.
Common Orthopaedic Procedures in India
Arthroplasty (Joint Replacement): Conservative estimates suggest that over 200,000 knee replacements are performed annually in India. While urban centers have high access to rehabilitation, a significant gap remains in semi-urban areas where post-operative follow-up is often neglected.
Arthroscopy and Sports Medicine: There is a surge in ACL reconstructions and meniscus repairs, yet clinical observations suggest that nearly 30% of these patients do not achieve full pre-injury functional levels due to unstructured rehab.
Spine Surgery: Decompressions and fusions for lumbar and cervical pathologies are common. Without structured core stabilization and postural re-education, the incidence of “adjacent segment disease” remains a concern.
Fracture Fixation: Rates of internal fixation for hip and long-bone fractures remain high due to road traffic accidents. Delayed mobilization in these cases often leads to permanent gait abnormalities.
The primary reason for failed recovery in these cohorts is not surgical failure, but rather a lack of coordinated care between the operating surgeon and the rehabilitating physiotherapist.

WHY STRUCTURED PHYSIOTHERAPY MATTERS AFTER SURGERY
The transition from a “surgical patient” to a “functional individual” requires a deep understanding of biological tissue healing.
Biological Timelines
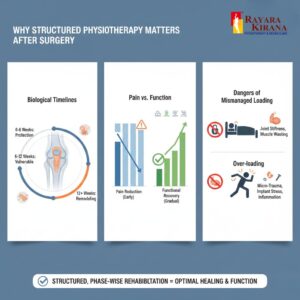
Bone healing (callus formation), tendon-to-bone integration, and ligamentization of grafts follow a strict chronological sequence. For instance, an ACL graft is at its weakest between 6 to 12 weeks post-surgery. A structured program ensures that the mechanical load applied does not exceed the structural integrity of the healing tissue.
Pain vs Function
Many patients equate the absence of pain with “recovery.” However, pain reduction is often achieved through medication and rest, whereas functional recovery—restoring muscle torque, proprioception, and joint kinematics—requires targeted stimulus.
The Dangers of Mismanaged Loading
Under-loading: Leads to joint capsule tightening, dense adhesions, and muscle wasting.
Over-loading: Causes micro-trauma to healing sites, increased inflammatory exudate, and potential loosening of hardware or sutures.
PHASE-WISE POST-SURGICAL PHYSIOTHERAPY FRAMEWORK
Phase 1: Immediate Post-Operative Phase (Protection & Circulation)
Goals: Control edema, prevent Deep Vein Thrombosis (DVT), and maintain range of motion (ROM) in adjacent joints.
Focus: Ankle pumps, isometric contractions, and respiratory physiotherapy.
Precautions: Avoid active-resisted movements of the operated site.
Red Flags: Excessive calf pain, shortness of breath, or foul-smelling discharge from the incision.
Early Mobility & Protection Phase
Goals: Restore basic ROM and initiate protected weight-bearing.
Focus: Closed-chain exercises, gait training with assistive devices, and scar tissue mobilization.
Precautions: Strict adherence to weight-bearing status (NWB/PWB/FWB) as prescribed by the surgeon.
Strengthening & Motor Control Phase
Goals: Restore 70-80% of muscle strength and improve neuromuscular control.
Focus: Progressive resistance training, balance exercises (proprioception), and correcting compensatory movements.
Precautions: Avoid ballistic movements or high-impact loading.
Functional & Activity-Specific Training
Goals: Return to specific daily tasks or light recreational activities.
Focus: Task-oriented training, advanced proprioception, and eccentric strengthening.
Return to Work / Sports / Daily Life
Goals: Full integration into pre-surgery lifestyle.
Focus: Plyometrics (for athletes), ergonomic training (for office workers), and long-term maintenance protocols.

SURGERY-SPECIFIC REHABILITATION CONSIDERATIONS
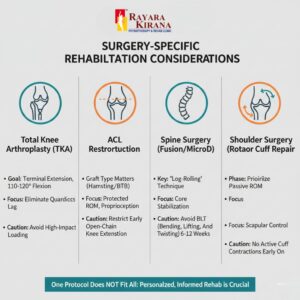
A “one-size-fits-all” approach is clinically dangerous.
Total Knee Arthroplasty (TKA): Focus is on achieving terminal knee extension and functional flexion (110°–120°) while ensuring quadriceps lag is eliminated.
ACL Reconstruction: The protocol must account for the type of graft used (Hamstring vs. BTB). Open-chain terminal knee extension is often restricted in early phases to protect the graft.
Spine Surgery (Microdiscectomy/Fusion): Emphasis is on “log-rolling” techniques and avoiding the “BLT” movements (Bending, Lifting, Twisting) for the first 6–12 weeks.
Shoulder Surgery (Rotator Cuff Repair): Protection of the repair is paramount; passive ROM is prioritized before any active engagement of the cuff muscles.
HIGH-RISK POST-SURGICAL PATIENT GROUPS
Certain populations require a more nuanced, cautious approach:
The Elderly: Higher risk of secondary complications like pneumonia or pressure sores. Rehab must focus on fall prevention and bone density.
Diabetic Patients: At increased risk for delayed wound healing and adhesive capsulitis (frozen shoulder) following any upper limb surgery.
Obese Patients: Increased mechanical stress on lower limb implants requires a focus on low-impact cardiovascular conditioning.
Athletes: Often prone to “over-rehabilitating,” these patients require psychological cues to respect healing timelines despite high motivation levels.
COMMON POST-SURGICAL COMPLICATIONS PREVENTED BY PHYSIOTHERAPY
Structured intervention serves as a preventative shield against:
Arthrofibrosis: Excessive scar tissue that locks the joint.
Muscle Atrophy: The rapid loss of muscle mass (especially VMO in the knee) that occurs within 48 hours of surgery.
Reflex Sympathetic Dystrophy (CRPS): Chronic pain caused by nervous system over-reactivity.
Gait Deviations: Trendelenburg gait or antalgic patterns that, if not corrected, lead to secondary hip or back pain.
WHEN PHYSIOTHERAPISTS MUST NOT PROGRESS OR MUST REFER BACK
Clinical safety is the cornerstone of Rayara Kirana Physiotherapy. Progression must be halted if:
Increasing Pain/Swelling: If pain scores increase and persist for >24 hours post-exercise.
Mechanical Symptoms: Sudden locking, clicking, or a “giving way” sensation.
Wound Dehiscence: Any opening of the surgical site or persistent drainage.
Neurological Deficit: New-onset numbness, tingling, or weakness in the distal limb.
Unexplained Calf Pain: Potential sign of Deep Vein Thrombosis.
STRUCTURED POST-SURGICAL PHYSIOTHERAPY DECISION PATHWAY
(Rayara Kirana Physiotherapy Internal Protocol)
STEP 1: Initial Presentation
Review Surgeon’s operative note and specific restrictions.
Assess wound status and neurovascular integrity.
STEP 2: Assessment of “The Big Three”
Pain: VAS Scale (Is it manageable?)
Swelling: Girth measurements (Is it localized or spreading?)
Mobility: Passive vs. Active ROM (Does it match the expected phase?)
STEP 3: Decision Node
IF Red Flags present (Fever, severe swelling, calf pain) → REFER BACK TO SURGEON.
IF Pain/Swelling is stable but ROM is restricted → HOLD STRENGTHENING, FOCUS ON MOBILIZATION.
IF Criteria for current phase are met → PROGRESS TO NEXT PHASE.
STEP 4: Execution
Apply phase-specific loading.
Educate caregiver on home-program safety.
CURRENT ADVANCES IN POST-SURGICAL REHABILITATION
Modern rehabilitation is moving toward “Pre-habilitation” (strengthening before surgery) and the use of technology. At our center, we emphasize:
Neuromuscular Electrical Stimulation (NMES): To combat arthrogenic muscle inhibition.
Blood Flow Restriction (BFR) Training: Allowing patients to gain muscle hypertrophy using very low loads, protecting healing joints.
Objective Outcome Measures: Using goniometry, dynamometry, and functional hop tests to ensure decisions are data-driven, not subjective.
EXPERT COMMENTARY
“The surgery is the ‘hardware’ update, but physiotherapy is the ‘software’ installation. Without structured rehab, even the most perfectly placed implant can fail due to abnormal loading or joint stiffness. I rely on my physiotherapy colleagues to be my ‘eyes’ during the months following discharge, ensuring that the biological integration of the surgery is never compromised.”
“Our role is to balance the ‘Art of Healing’ with the ‘Science of Loading.’ We don’t just give exercises; we manage the physiological response of the body to the trauma of surgery. Safety is not about moving less; it is about moving correctly at the right time. Our priority is protecting the surgeon’s work while restoring the patient’s life.”
FAQ : EVERYTHING YOU NEED TO KNOW
When should physiotherapy start after surgery?
Usually within 24 hours for circulation and basic mobility, unless specified otherwise by your surgeon.Can physiotherapy damage my new implant?
If performed under professional supervision following a structured protocol, no. It actually protects the implant by stabilizing the surrounding muscles.Is pain normal during physiotherapy?
Mild discomfort is expected, but sharp, stabbing, or escalating pain is a signal to stop and reassess.How long does recovery really take?
While initial healing takes 6-12 weeks, full functional recovery often takes 6-12 months depending on the surgery.Can I just do the exercises at home using YouTube?
No. YouTube cannot assess your swelling, scar tissue quality, or compensatory movements. This often leads to secondary injuries.Why is my joint stiff in the morning?
This is often due to post-surgical inflammation and fluid accumulation. Guided movement helps “flush” the joint.Do I need physiotherapy if I can already walk?
Walking is just one function. You need rehab for balance, stair climbing, and preventing future joint wear.What is “Pre-hab”?
Physiotherapy before surgery to optimize muscle strength, which significantly speeds up post-op recovery.How often do I need to visit the clinic?
Initially 3-5 times a week, tapering down as you gain independence and safety in your home program.What happens if I skip my sessions?
You risk permanent stiffness, muscle weakness, and a higher chance of needing a “manipulation under anesthesia.”Can I drive after my surgery?
This depends on the limb operated on and your reaction time. Your PT will perform specific tests to clear you for driving.Will ice or heat help more?
In the early post-op phase, ice is generally used to control inflammation. Heat is reserved for later stages to relax muscles.Why is my “good” leg hurting?
Because you are overcompensating. Structured rehab focuses on restoring symmetry to protect your non-operated joints.Is it okay to take pain killers before physiotherapy?
Discuss this with your doctor. While it helps movement, we don’t want to mask pain that serves as a safety warning.What are “precautions” after hip surgery?
Specific movements like crossing your legs or bending past 90 degrees that could cause the new joint to dislocate.How do I know if my wound is infected?
Look for increased redness, warmth, persistent oozing, or a fever.When can I return to sports?
Only after passing specific functional tests (strength, hop tests, agility) to ensure your risk of re-injury is low.Can I use a massage gun on my surgical site?
Never directly on the incision or healing bone. Consult your PT for safe soft-tissue release techniques.Why do I feel “tired” after a simple session?
Surgery and healing consume significant metabolic energy. Fatigue is a normal part of the systemic recovery process.Is physiotherapy a “luxury” or a “necessity”?
In post-surgical cases, it is a clinical necessity to ensure the surgical goal is achieved.
CONCLUSION
Post-surgical recovery is a delicate journey that requires a bridge between surgical precision and functional movement. At Rayara Kirana Physiotherapy, we believe that structured, phase-wise rehabilitation is the only path to a safe and lasting recovery. By respecting the biological timelines of healing and maintaining a rigorous, safety-first approach, we ensure that our patients do not just “get better,” but return to their lives with strength, confidence, and resilience. Collaborative care between the surgeon, the therapist, and the patient is the gold standard for long-term success.