The hamstring is perhaps the most misunderstood muscle group in the human body.
Often relegated to a simple “leg day” accessory or a target for basic stretching, the hamstrings are actually high-performance instruments that act as the primary brakes and stabilizers for the lower body.
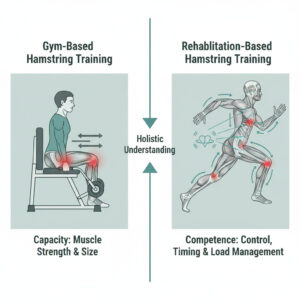
The common misconception is that a “strong” hamstring is a “safe” hamstring. Yet, sports medicine clinics are filled with athletes who can deadlift double their body weight but still suffer recurrent Grade 2 tears. This paradox exists because gym training focuses on capacity, while physiotherapy focuses on competence.
If you are returning to the gym after a “tweak” without clinical rehabilitation, you aren’t just training your muscles—you are likely training a compensation pattern that will eventually lead to chronic pain or reinjury. This guide explores why clinical rehab is a form of neuromuscular re-education that a standard gym workout simply cannot replicate.
Understanding the Hamstring Beyond Muscle Strength
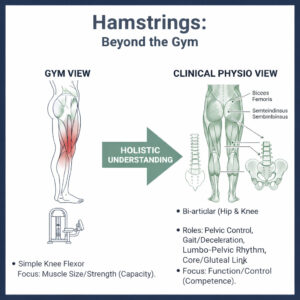
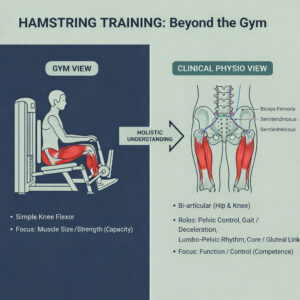
In a gym setting, hamstrings are often viewed as simple knee flexors. Clinically, they are far more complex. The hamstrings are bi-articular, meaning they cross two joints: the hip and the knee.
This dual-joint nature means they are responsible for:
Pelvic Control: They act as a tether for the pelvis, preventing excessive anterior tilt.
Gait and Deceleration: During running, the hamstrings must fire eccentrically (lengthening under tension) to slow the leg down before the foot hits the ground.
Lumbo-pelvic Rhythm: They coordinate with the gluteals and lower back to ensure the spine moves safely during bending.
When you use a seated leg curl machine, you isolate the muscle. However, in real life, the hamstring never works in isolation. It functions as part of a posterior chain including the glutes, adductors, and even the calf-ankle complex. If your ankle is stiff or your glutes are “sleepy,” the hamstring is forced to overwork, leading to the “tightness” many people mistakenly try to stretch away.
How Gyms Typically Train Hamstrings (and Their Limitations)
Standard gym programming is built on the principles of hypertrophy (growth) and absolute strength. While movements like Romanian Deadlifts (RDLs) and Nordic Curls are excellent for building tissue bulk, they often overlook the “how” of the movement.
What Gym Workouts Usually Lack:
Neural Tension Assessment: Is the “tightness” a short muscle, or is it the sciatic nerve being tethered?
Pelvic Asymmetry: Most gym-goers favor one side without realizing it, leading to one hamstring bearing 60-70% of the load.
Eccentric Quality: Many can lift a heavy weight but lack the control to lower it slowly without their pelvis tilting or their lower back arching.
Gym training is performance-oriented. Rehab is injury-aware. In the gym, the goal is to move the weight; in rehab, the goal is to move the body correctly under the weight.
How Physiotherapists Clinically Assess Hamstrings
When you see a physiotherapist, we don’t just ask how much you can lift. We look at load intelligence.
Our assessment includes:
Lumbo-pelvic Stability: Can you maintain a neutral spine while the hamstring is under tension?
Neural Mobility: We test the sliding capacity of the sciatic nerve. If the nerve doesn’t slide, the muscle will stay “tight” as a protective mechanism.
Fatigue Patterns: We observe how your movement changes when you are tired. Most injuries happen in the last 15 minutes of a game, not the first.
Pain-Free Strength vs. Readiness: Just because it doesn’t hurt to squeeze a ball between your legs doesn’t mean your hamstring is ready to handle a 20mph sprint.
Rehab-Based Hamstring Training – What People Don’t Know
The “secret sauce” of physiotherapy isn’t the exercises themselves, but the timing and motor control.
Motor Control vs. Muscle Power:
You can have a powerful engine, but if the timing belt is off, the car won’t run. We retrain the brain to fire the hamstring at the exact millisecond required during the “swing phase” of running.
Phase-Based Loading:
Early in rehab, we avoid heavy stretching because it can pull apart healing fibers. Instead, we use isometrics (holding tension without movement) to bridge the gap between injury and active exercise. Gyms often skip this, moving straight to heavy loading, which creates “patchwork” scar tissue that is prone to re-tearing.
Role of Neuromuscular Re-education
After an injury, the brain develops a “fear response.” It may “switch off” parts of the hamstring to protect it (reflex inhibition). This is why your leg might feel “weak” even if the muscle looks large.
Physiotherapy uses proprioceptive training—challenging the muscle’s sense of position in space. We use unstable surfaces, reactive drills, and cognitive distractions to ensure that your hamstring can protect itself even when you aren’t thinking about it.
Use of Physiotherapy Modalities
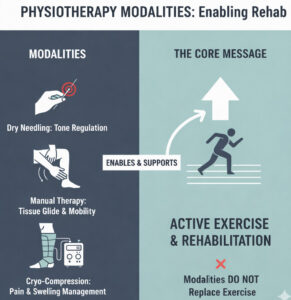
Modalities are the “enablers” of rehab. They don’t make you strong, but they create the environment for strength to happen.
Dry Needling: Used to reset muscle tone and release “trigger points” that cause referred pain.
Manual Therapy: Used to ensure the various layers of muscle and fascia “glide” over each other rather than sticking together.
Cryo-compression: Tools like Game Ready help manage the inflammatory window, allowing for earlier pain-free movement.
Why Rehab Progression Is Phase-Based
Unlike a gym program that might change every 4-6 weeks based on gains, rehab changes based on tissue biology:
Acute Phase: Protection and pain management.
Sub-acute Phase: Restoring range of motion and initiating low-load isometric work.
Remodeling Phase: Building eccentric strength and ensuring the new fibers align correctly.
Return-to-Function: Sport-specific drills and high-velocity loading.
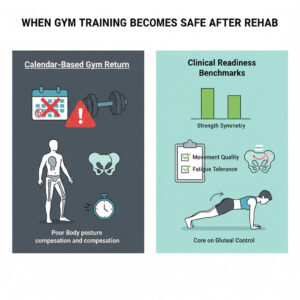
When Gym Training Becomes Safe After Rehab
You are ready for the gym when you meet Clinical Benchmarks, not just when the calendar says so.
Symmetry: Within 5-10% strength of the uninjured side.
Quality: Zero compensation in the pelvis during a single-leg bridge.
Fatigue: Ability to maintain form during high-repetition endurance tests.
Common Mistakes Patients Make
The “No Pain, All Gain” Trap: Assuming that because it doesn’t hurt, it’s healed.
Stretching the “Tightness”: Often, hamstrings feel tight because they are overstretched/weak due to an anteriorly tilted pelvis. Stretching makes this worse.
Skipping the Glutes: The glutes are the hamstring’s best friend. Training one without the other is a recipe for disaster.
Doctor’s Expert Comments
Dr. Kiran S. Murthy, PT
“In my thirty years of practice, the biggest tragedy is the ‘phantom recovery.’ An athlete feels strong in the gym, does a heavy deadlift, and thinks they are cured. But gym strength is linear. Real-world injury happens in the non-linear moments—the sudden deceleration or the slip. Without clinical rehab to address these reactive phases, the muscle is essentially a powerful engine with no brakes.”
Dr. Yoginder Balaji, PT
“We must look at the pelvis. The hamstring is a slave to pelvic position. If your physical therapist isn’t assessing your core and pelvic tilt, they aren’t treating your hamstring. Gym workouts focus on the muscle belly; clinical rehab focuses on the ‘control center’ that governs how that muscle is used.”
Dr. Bhavana, PT
“Recurrent hamstring issues are rarely just about the hamstring. They are the body’s way of screaming that the kinetic chain is broken. By the time you feel it in your hamstring, your lower back is often already compensating. Proper rehab stops the ‘domino effect’ that leads to chronic hip and disc issues five years down the line.”
Patient FAQs
Why did my hamstring injury return despite gym workouts?
You likely built strength without restoring neuromuscular timing and eccentric control.Is hamstring tightness the same as weakness?
Often, yes. A weak muscle stays in a state of high tone (feeling tight) to protect itself.Can deadlifts replace physiotherapy?
No. Deadlifts are a great capacity builder, but they don’t address neural tension or side-to-side imbalances.Does pain-free exercise mean my hamstring is healed?
No. Pain usually subsides long before the tissue has regained its original structural integrity.Can dry needling strengthen my hamstring?
No, it regulates muscle tone and reduces pain, making it easier for you to perform strengthening exercises.When should I stop gym training during hamstring pain?
If you experience sharp pain, a “pulling” sensation that lingers, or pain that increases the morning after a workout.Why do I feel pain near the sitting bone?
This is often Proximal Hamstring Tendinopathy, which requires a specific loading protocol different from a mid-muscle tear.How long does true hamstring rehab take?
Depending on the grade, anywhere from 6 weeks to 6 months for full, high-speed athletic return.Can improper hamstring training cause back pain?
Absolutely. A dysfunctional hamstring forces the lower back to overwork during bending movements.Do runners need different hamstring rehab?
Yes. Runners require high-speed “swing phase” eccentric training that a bodybuilder wouldn’t necessarily need.What is the ‘Nordic Curl’ and is it enough?
It’s a great eccentric exercise, but it’s only one piece of the puzzle.Should I use ice or heat?
Ice for the first 48-72 hours for pain; heat later to promote blood flow for healing.Is walking good for a hamstring strain?
Gentle walking is good for blood flow, but limping is a sign you are overdoing it.Why does my hamstring hurt when I sit?
This is a classic sign of tendon involvement near the ischial tuberosity (sitting bone).Can I play through a ‘minor’ strain?
Doing so often turns a 2-week recovery into a 3-month chronic issue.What is ‘eccentric’ training?
Training the muscle while it is lengthening (e.g., the lowering phase of a leg curl).Why do physios check my ankles for a hamstring issue?
Stiff ankles change your gait, which can put excessive force on the hamstrings.Can I use a foam roller?
It can help with temporary relief, but it won’t “fix” a tear or weakness.What is neural flossing?
A technique used by physios to ensure the sciatic nerve moves freely through the muscle.Is surgery ever needed for hamstrings?
Only in rare cases of complete “avulsion” (the muscle tearing off the bone).
Conclusion
The gym is where you go to build a bigger, stronger body. Physiotherapy is where you go to ensure that body actually works. When it comes to the hamstrings, skipping the clinical rehab phase is like putting a Ferrari engine in a car with wooden brakes. You might go fast for a moment, but the crash is inevitable.
True recovery requires more than just sets and reps; it requires an understanding of anatomy, neurology, and biology. Respect the process, and your hamstrings will respect the load.